Sarin Poisoning on Tokyo Subway
SADAYOSHI OHBU, MD, AKIRA YAMASHINA, MD, NOBUKATSU TAKASU, MD, TATSUO
YAMAGUCHI, MD, TETSUO MURAI, MD, KANZOH NAKANO, MD, YUKIO MATSUI, MD, RYUZO
MIKAMI, MD, KENJI SAKURAI, MD, and SHIGEAKI HINOHARA, MD, Tokyo, Japan
ABSTRACT: On the day of the disaster, 641 victims were seen at St. Luke's International Hospital. Among those, five victims arrived with cardiopulmonary or respiratory arrest with marked miosis and extremely low serum cholinesterase values; two died and three recovered completely. In addition to these five critical patients, 106 patients, including four pregnant women, were hospitalized with symptoms of mild to moderate exposure. Other victims had only mild symptoms and were released after 6 hours of observation. Major signs and symptoms in victims were miosis, headache, dyspnea, nausea, ocular pain, blurred vision, vomiting, coughing, muscle weakness, and agitation. Almost all patients showed miosis and related symptoms such as headache, blurred vision, or visual darkness. Although these physical signs and symptoms disappeared within a few weeks, psychologic problems associated with posttraumatic stress disorder persisted longer. Also, secondary contamination of the house staff occurred, with some sort of physical abnormality in more than 20%.ON MARCH 20, 1995, terrorists released sarin, an organophosphate (OP) nerve gas at several points in the Tokyo subway system, killing 11 and injuring more than 5,500 people.
Sarin is one of OP anticholinesterase compounds. Other nerve agents include tabun, soman, and VX gas. These chemical warfare agents have caused accidental exposure to military personnel. We report on the second sarin gas incident involving civilians after the first Matsumoto sarin incident1 in which the same terrorist group killed seven and injured more than 200 people.
Pure sarin is colorless, odorless, and volatile, and a highly lethal OP compound. Its pathogenic mechanism is to inhibit the enzymatic action of cholinesterase (ChE), producing excessive amounts of acetylcholine which, in turn, causes signs and symptoms mainly in muscarinic, nicotinic, and central nervous system structures.2-5 Sarin can be absorbed through any body surface, but vaporized sarin is mainly absorbed through the respiratory tract and conjunctiva. Since most victims encountered vaporized sarin, they showed ophthalmic and respiratory signs and symptoms.
On the day of the sarin release, 641 patients were seen at St. Luke’s International Hospital (SLIH) and 349 were seen in the following week (Table 1). Thus, SLIH treated the largest reported patient population exposed to sarin.
DETAILS OF THE INCIDENT
The nerve gas sarin was released in commuter trains on three different Tokyo subway lines by a terrorist cult group. Sarin was concealed in lunch boxes and soft-drink containers and placed on subway train floors. It was released as terrorists punctured the containers with umbrellas before leaving the trains. The incident was timed to coincide with rush hour, when trains were packed with commuters. Over 5,500 were injured in the attack. A subway station close to SLIH was one of several sites hit simultaneously in the attack; therefore, many of the victims were sent to SLIH.
CLASSIFYING THE INJURED
We classified victims into three categories: mild severity patients were principally mobile and their symptoms were mainly eye problems related to miosis, rhinorrhea, and mild headache; moderate severity was indicated if victims were immobile or complained of moderate degree dyspnea, vomiting, severe headache or with neurologic complication like fasciculation; critical was indicated if victims had cardiac or respiratory arrest.
Critical Category
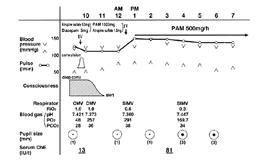
Of the 641 patients seen at SLIH on the day of the disaster, five were in critical condition. Three patients had cardiopulmonary arrest (CPA) and two were unconscious and had respiratory arrest soon after arrival (Table 2). Of these five critically ill patients, three were successfully resuscitated and able to leave on hospital day 6. One CPA patient did not respond to cardiopulmonary resuscitation (CPR) and died with findings of conspicuous miosis that continued even at the time of her death. A second patient with CPA was resusci- tated but died on hospital day 28 due to irreversible brain damage. This patient had markedly decreased serum ChE level of 6 IU/L (reference value: 100 IU/L to 250 IU/L). The third CPA patient, a 21-year-old woman who collapsed while attempting to leave the subway (Fig 1), was brought to our emergency center. She responded to CPR and a spontaneous heart beat returned within 5 minutes. A generalized convulsive seizure 1 hour later ceased after 5 mg of intravenous diazepam. After the administration of an initial 1 g and a subsequent 0.5 g per hour of pralidoxime iodide (PAM) intravenously, the victim regained consciousness within 30 minutes and started breathing spontaneously within 4 hours. At 4 PM, her pupils were 3 mm in diameter. The initial serum ChE value of 13 IU/L increased to 81 IU/L at 3 PM. Total doses of 5 mg of atropine sulfate and 8.5 g of PAM were administered intravenously. The patient was discharged intact on hospital day 6 (Fig 1). The fourth and fifth critical patients were drowsy when brought to the emergency center; several minutes later, both had generalized convulsions and lapsed into respiratory arrest. Intravenous diazepam injections and mechanical ventilation improved neurologic status and they soon recovered spontaneous breathing. The fourth patient was discharged on day 3 (Fig 2) and the fifth on day 4.
Initial treatment for these critically ill patients included CPR, 2 mg of intravenous atropine sulfate, and 5 mg to 20 mg of intravenous diazepam for convulsive disorders. After learning that sarin gas was responsible for the patients’ symptoms, we added intravenous PAM to this regimen. In view of the patients’ peculiar signs of miosis and markedly decreased serum ChE levels, an OP compound was suspected to be the causative agent and PAM was initiated in two cases before sarin was identified as the causative agent.
Moderate Category
On the day of the attack, we decided overnight observation was needed if patients showed signs and symptoms other than eye problems or mild headache after the first 6-hour observation. Thus, 106 patients were hospitalized with moderate severity for overnight observation. There were 43 men and 63 women whose ages ranged from 13 years to 60 years. They included four pregnant women. Miosis was the most common sign present in 105 patients, most with pupils of less than 1 mm in diameter. Other ophthalmologic symptoms were ocular pain, blurred vision, and visual darkness. Many patients had headache, particularly with near vision. Dyspnea, nausea, vomiting, muscle weakness, coughing, agitation, and fasciculation were relatively common (Table 3). Hospitalized patients were treated initially with 2 mg of intravenous atropine sulfate and 2 g of PAM after the causative agent was confirmed to be sarin. Intravenous diazepam was given for fasciculation. All but five patients were discharged by hospital day 5. In nearly all patients hospitalized, symptoms other than those related to miosis (eg, ocular pain, blurred vision, and visual darkness), improved by the time of discharge. Miosis was severe and persistent, showing unresponsive to intravenous atropine sulfate and continuing over 1 week unless mydriatic agents were applied locally. Commercial eye drop mixtures of 0.5% tropicamide and 0.5% phenylephrine hydrochloride or 1% cyclopentolate hydrochloride relieved miosis and associated symptoms. Headache and malaise were the most common, persistent generalized symptoms noted after discharge from the hospital. Some patients also mentioned anxiety, fear, nightmares, insomnia, and irritability; of these, five had nightmares and insomnia so severe that they required visits to psychiatrists.
Mild Category
The remaining 531 patients, mainly with eye problems, were treated in the outpatient department waiting room and released after 6 hours of observation. Intravenous atropine sulfate, in doses of up to 2 mg had no effect in these patients. Some patients complained of palpitations after atropine sulfate administration, and one had chest pain and pupil dilation remained unchanged.
Pregnant Patients
Four pregnant women, between 9 weeks’ and 36 weeks’ of gestation, were admitted to the obstetric ward. All had miosis, headache, nausea, and vomiting, with slightly decreased ChE levels between 72 IU/L and 99 IU/L. One woman had a healthy baby 3 weeks after the incident. The three others also had healthy babies without complication. The pregnant women we saw in the incident did not attempt to terminate pregnancy and the course of their pregnancies was unaffected.
LABORATORY DATA
A histogram of serum ChE levels measured by 5-5' dithiobis (2-nitrobenzoic acid) [DTNB] method from blood samples taken a few hours after sarin exposure in the 451 hospitalized patients and outpatients were shifted to the left (Fig 3). About half of the patients showed decreased ChE levels a few hours after exposure. All severely ill patients showed markedly decreased ChE levels and 74% of admitted patients showed decreased ChE levels. When we compared serial changes in serum ChE levels in those who were treated with larger doses of PAM (3 g or more) to those who were treated with smaller doses of PAM (less than 3 g) among admitted patients, there was a tendency for serum ChE levels to improve faster in the group receiving larger doses. Although not conclusive, this suggests that PAM increases serum ChE levels. The white blood cell count was increased in 60% of the victims and creatine phosphokinase was increased in 11%. Arterial blood gas analyses showed respiratory alkalosis in 67% of hospitalized patients. Other routine tests were within normal ranges. Electrocardiograms in admitted patients revealed no significant or specific abnormalities.
HOSPITAL DEPLOYMENT
To aid the house staff in achieving and maintaining a proper level of disaster preparedness, SLIH conducts routine disaster drills. The nerve gas attack was so unprecedented in nature and site, however, that management guidelines were inadequate; we had no means of handling such an extraordinarily large number of simultaneously affected patients. A headquarters was organized to collect and process information, and instructions were distributed on how to treat patients. Victims were advised to remain in the hospital and receive intravenous drip infusions until the causative agent and its therapy could be ascertained. All patients remained in the hospital for observation for at least 6 hours. Those seriously ill were transferred directly to intensive care, and those with disturbances of vital signs or neurologic or psychologic abnormalities were advised to remain in the hospital for 24-hour observation. The remaining 530 patients, mainly suffering eye problems, were treated and released after 6 hours of observation in the outpatient department waiting room. No instructions were given, unfortunately, on the prevention of secondary contamination.
POST-INCIDENT SYMPTOMS
Many victims had post-incident symptoms (Table 4). According to questionnaires distributed to 610 victims seen at SLIH (return rate: about 80%), almost 60% of respondents still suffered from some post-incident symptoms, which can be indication of posttraumatic stress disorders (PTSD), 1 month after the incident. This percentage remained almost the same even 3 and 6 months after the incident. Fear was seen in 32% of the victims, some of whom still cannot use the subway. Insomnia was seen in 29%. Sixteen percent had flashbacks of the terrible scenes they had witnessed. Some patients become depressed (16%) or irritated (16%). Nightmares persisted in 10%. A typical nightmare involves the appearance of big monsters or huge rocks falling on victims. Headache and malaise are the most common generalized post-incident symptoms. Even several months after the incident, many patients still suffer from PTSD, diagnosed by the criteria of DSM-IV,6 and must seek the service of psychiatrists.
SECONDARY CONTAMINATION AT HOSPITAL
Secondary contamination of house staff who treated victims cannot be ignored. Since no information that the incident was caused by poison gas was available in the first few hours of the attack, sarin gas decontamination was not attempted, so a certain percentage of house staff showed signs of sarin poisoning. Questionnaires were given to the entire hospital staff (1,063 people, return rate: 45%), and the results revealed that 23% had some sort of physical disorder, though mild. Over 20% of house staff who treated victims had symptoms that included ocular pain, headache, sore throat, dyspnea, nausea, dizziness, and nose pain, but none was seriously affected (Fig 4).
DISCUSSION
The most common signs and symptoms were miosis and miosis-related symptoms such as visual darkness. Almost all victims showed ocular disorders, including marked miosis, ocular pain, headache especially with near vision, and blurring of vision. Major respiratory symptoms were rhinorrhea, cough, and dyspnea. Severely ill victims had respiratory failure due to central nervous system involvement, a nicotinic effect on the respiratory muscles, and/or the muscarinic effect on the smooth muscle and secretory glands of the airway, resulting in bronchoconstriction and excess bronchial secretion. An impressive phenomenon was noted in two patients who went into respiratory arrest shortly after becoming unconscious and having convulsive seizure. They were successfully resuscitated and became fully conscious but unable to breathe.
The difference in the severity among victims was probably a result of the size of the dose inhaled, although we could not estimate the dose, the exposure-time, or the distance from the source. We can easily imagine that the larger the dose inhaled, the more severe the complications manifested. However, in emergency situations, we have to diagnose clinically this kind of intoxication by totally considering history of exposure, clinical signs and symptoms, and serum ChE because no definitive diagnostic examination is available in ordinary clinical situations. Since sarin is one of the highly lethal OP compounds, a higher percentage of victims could have died in this incident. In contrast, an overwhelming majority suffered only mild symptoms. We therefore surmise that the sarin used was diluted.
We initially attempted to relieve symptoms by administering intravenous atropine sulfate, but the intravenous route was not effective in counteracting miosis. Its topical application was effective, in contrast, but some patients had lingering side effects causing further visual problems due to resulting mydriasis. We found that patients tolerated repeated applications of commercial eye drops, which combined tropicamide and phenylephrine hydrochloride or cyclopentolate hydrochloride. Intravenous administration of atropine sulfate to mildly ill victims was adverse. We believe that it was because eye symptoms were mainly due to local reaction of sarin. Intravenous PAM was initiated after we learned sarin gas was the causative agent. The principal mode of action of PAM, the only oxime available in Japan, is to displace the nerve agent that binds to ChE. We therefore recommend that PAM be administered before the ChE bound to the sarin ages. It is our clinical impression that we could have managed the signs and symptoms of almost all of our mildly affected patients without PAM, but patients in critical condition seemed to have benefitted from PAM, which suppressed muscle fasciculation and restored normal serum ChE levels.
As described in the Laboratory Data section, there is a relationship between the value and the clinical severity when we consider patients as a group, but actually there were some patients with low ChE presenting only mild symptoms. At present, there are no patients who show significant delayed side effects, including intermediate syndrome or rebounding symptoms, which have been seen in other OP intoxication cases. So, in acute phase of treatment, the most reliable predictor of outcome is the clinical status at 3 hours to 5 hours after the exposure including respiration, circulation, and consciousness level. Once the patient survives for a few hours, the prognosis is equally as good as that of unexposed people.
Psychologic complications cannot be disregarded; almost 60% of victims suffered from PTSD that persisted longer than 6 months. Psychiatric consultation has been required for many victims.
Secondary contamination of house staff can also be a major problem. Some of our staff showed miosis and complained of nose and throat congestion. In confronting suspected nerve gas poisoning, decontamination of the causative agent and highly effective ventilation of rooms are critical.
Japan has had no previous experience with this form of terrorism. We are now aware of the extent to which governments of other countries have developed emergency plans to cope with terrorism. The aid and advice provided by the international community to cope with this disaster was greatly appreciated. One of the major lessons we have learned is the importance of worldwide cooperation among health care professionals in managing and overcoming incidents of this magnitude.
References
1. Morita H, Yanagisawa N, Nakajima T, et al: Sarin poisoning in Matsumoto, Japan. Lancet 1995; 346:290-293
2. Marrs TC, Maynard RL: Neurotoxicity of chemical warfare agents. Handbook of Clinical Neurology. de Wolff FA (ed). Amsterdam, Elsevier, Vol 20, 1994, pp 223-235
3. Sidell RF: Soman and sarin. clinical manifestations and treatment of accidental poisoning by organophosphates. Clin Toxicol 1974; 7:1-17
4. Gunderson CH, Lehmann CR, Sidell RF, et al: Nerve agents: a review. Neurology 1992; 42:946-950
5. Grob D: The manifestation and treatment of poisoning due to nerve gas and other organic phosphate anticholinesterase compounds. Arch Intern Med 1956; 98:221-239
6. American Psychiatric Association: Posttraumatic stress disorder. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC, American Psychiatric Association, 4th Ed, 1994, pp 424-429
Back to June INDEX
{kind=link}
{kind=link}
{kind=link}
{kind=link}